


Many people are struggling to get the dental care and treatment they need, says the independent watchdog of NHS services in Wales.
Reports undertaken by Community Health Councils (CHCs) across Wales (e.g. Swansea Bay CHC and Hywel Dda CHC) say that finding an NHS dentist for many people is “impossible”. They say this is having a significant impact on people’s dental health, with many feeling the pressure to pay privately or have no treatment at all.
There will be different views on what access to dentistry means among professionals and in terms of what the public/ patients might mean or value.
In a series of two articles, we will look at access to dentistry through an equality lens. This first article looks at which groups are struggling to access services. Our second article will look at prevention and access to community dental programmes.
Reduced access to dental care
Access to dental services has been severely impacted by the COVID-19 pandemic, and it is likely to take some time to deal with the backlog of patients in need of dental care and treatment.
The British Dental Association (BDA) Wales says that nearly two million treatments were lost during 2020-21.
The General Dental Council (GDC) explains that only urgent services were available during the first national lockdown. Since reopening in June 2020, dentists have reported reduced capacity due to further closures and the need for infection control measures, such as additional cleaning and fallow time.
The media reported instances where patients have been forced to carry out their own dentistry – buying temporary filling kits and treating themselves because practices couldn’t provide appointments.
Figure 1 (below) shows the impact of the pandemic on dentistry. The BDA warn that:
…patients across Wales will now inevitably face worse outcomes, with opportunities lost to act on the early signs of tooth decay, gum disease and even oral cancer.
But it also shows that only around 55 per cent of the population were able to access NHS dental care, even before the pandemic. It’s unknown which groups in the population were getting regular check-ups and which groups were struggling to access services and treatment.
Figure 1: Percentage of the population accessing NHS dental care within the recommended 2 year check-up period ¹
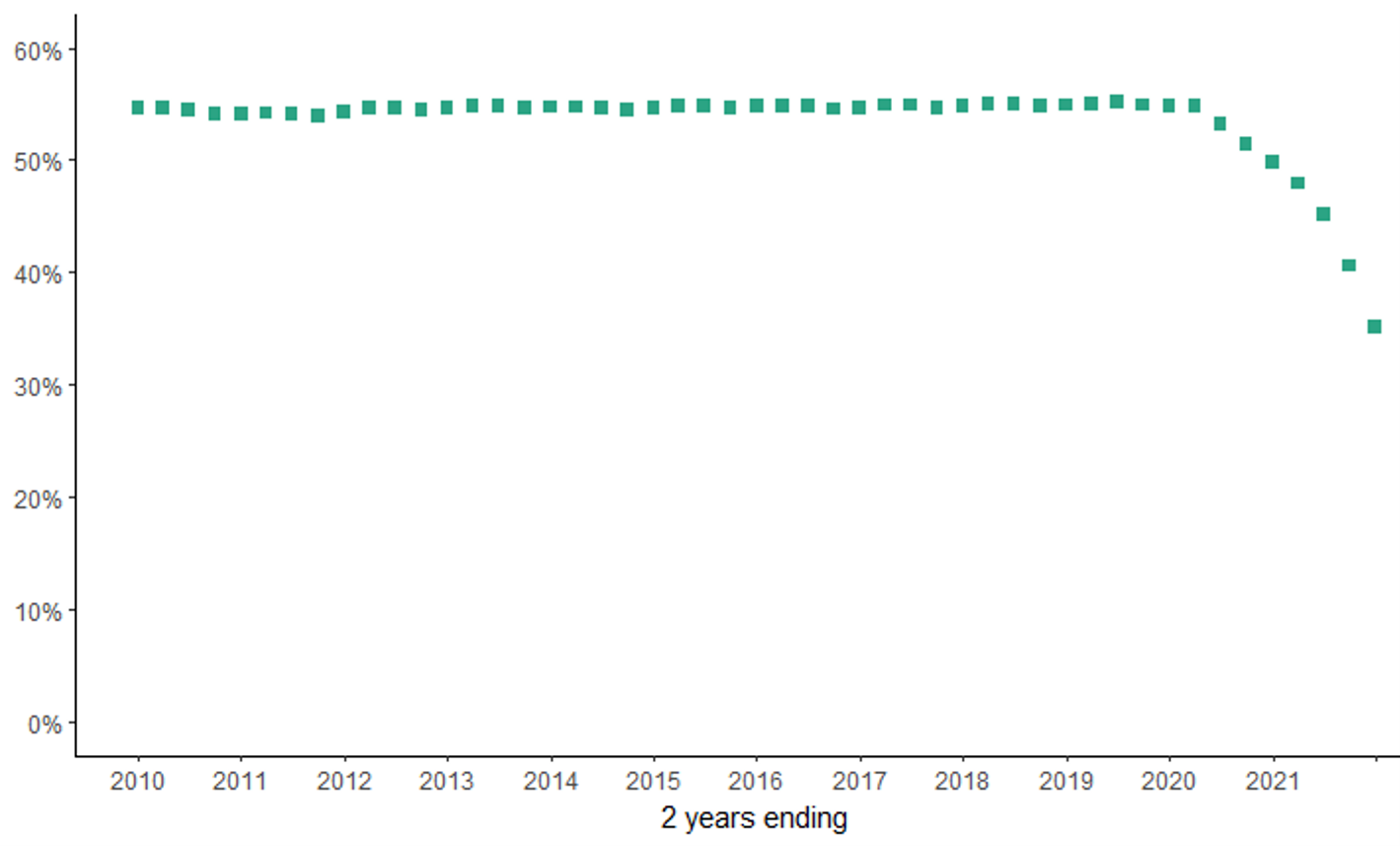
Source: StatsWales, NHS patients treated for adults and children by local health board.
¹ Data is provided quarterly and refers to the percentage of the population who went to the dentist at least once in the preceding two years.
Dental treatments are split into bands depending on the level of complexity, which also determines the cost:
- Band 1 includes examinations and simple treatments, such as x-rays and scale and polish;
- Band 2 includes more clinical procedures such as fillings, extractions and root canals;
- Band 3 includes more complex treatments (e.g. crowns, bridges and dentures); and
- Urgent refers to emergency, short term treatment to stop pain or prevent further deterioration.
Figure 2 shows that dental services have been slow to recover. Between October and December 2021 the number of Band 1 courses of treatment (which includes routine check-ups) was 70% lower than the 2009-2019 average for the same period.
Figure 2: Number of courses of dental treatment given to adults quarterly 2009-2021 by treatment band

Source: StatsWales, Courses of treatment by treatment band, patient type, local health board and quarter.
The impact is also felt in secondary care, where there are a range of dental specialities. The Welsh Government publishes data on this via StatsWales (see Figure 3):
- Oral surgery; concerned with surgery to the teeth, jaws and gums;
- Paediatric dentistry; look after children’s complex dental needs;
- Orthodontics; provide braces to straighten teeth and mainly provide services for children on the NHS;
- Restorative dentistry; focused on the management of diseases of the oral cavity, teeth and supporting structures; and
- Dental medicine; a branch of oral health
The latest data shows the number of patient pathways waiting to start treatment increased for all specialities except restorative surgery between April 2021 and April 2022. While the percentage of patients waiting over 36 weeks for treatment decreased for most specialities (except dental medicine) over this period, waiting times remain high for orthodontic treatment,dental medicine and oral surgery.In April 2022, 50% of patients had been waiting over 36 weeks for oral surgery.
Figure 3: Number of patient pathways waiting to start hospital treatment in April 2022 compared to April 2021 by dental speciality and waiting time.
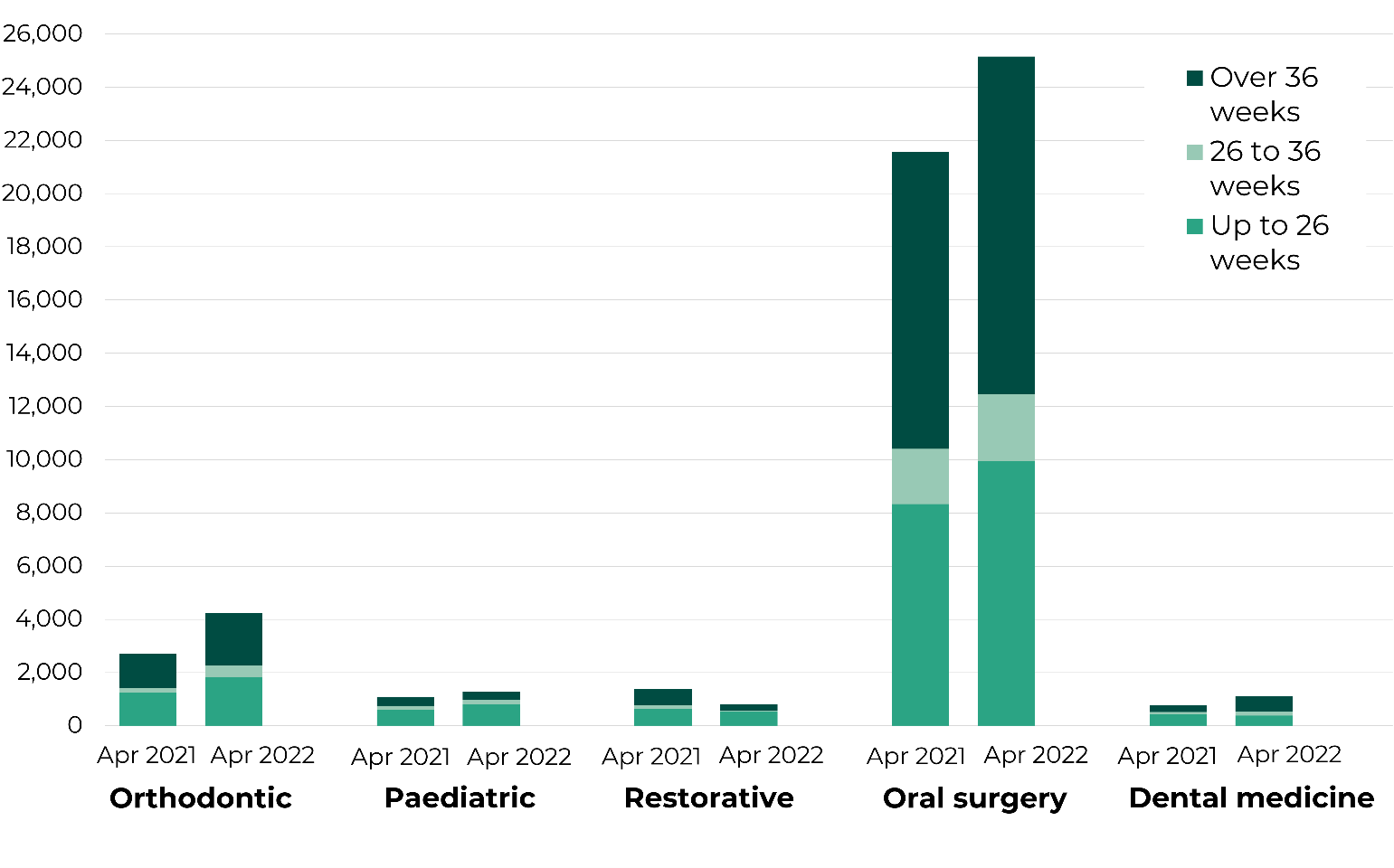
Source: StatsWales, Patient pathways waiting to start treatment by month, grouped weeks and treatment function, January 2021 onwards
Recovery of dental services
Two years on from the beginning of the pandemic, Swansea Bay CHC reported in February 2022 that a significant number of people are still unable to access NHS dental care and treatment. It says practices either have no available appointments, or are not taking on new NHS patients.
The Welsh Government set an expectation for 2021/22 that all NHS dental practices have a responsibility to see new patients. But there’s limited data on what services are available to the public and patients. In Plenary on 5 July, the First Minister said;
… our ambition is to make sure that there is NHS dentistry available to everybody who wishes to take it up.
Oral health inequalities
There’s very little information on which sections of the population are either unwilling, or unable to access dental services. Some people may choose to access private dentistry.
Research published by the GDC highlights that dental professionals are concerned that the decrease in dental capacity has most likely affected:
- Those who were extremely clinically vulnerable to COVID-19 (54%);
- People unable to afford dental treatment (48%); and
- Older people (43%).
Data shows that 16 NHS dental practices in Wales closed between July 2021 and June 2022. As practices close some people will need to travel further to access dental treatment, creating particular difficulties for people in rural areas, with limited mobility or on low-incomes.
Figure 4: Proportion of population within various travel distances to their nearest dentist by rurality and deprivation level
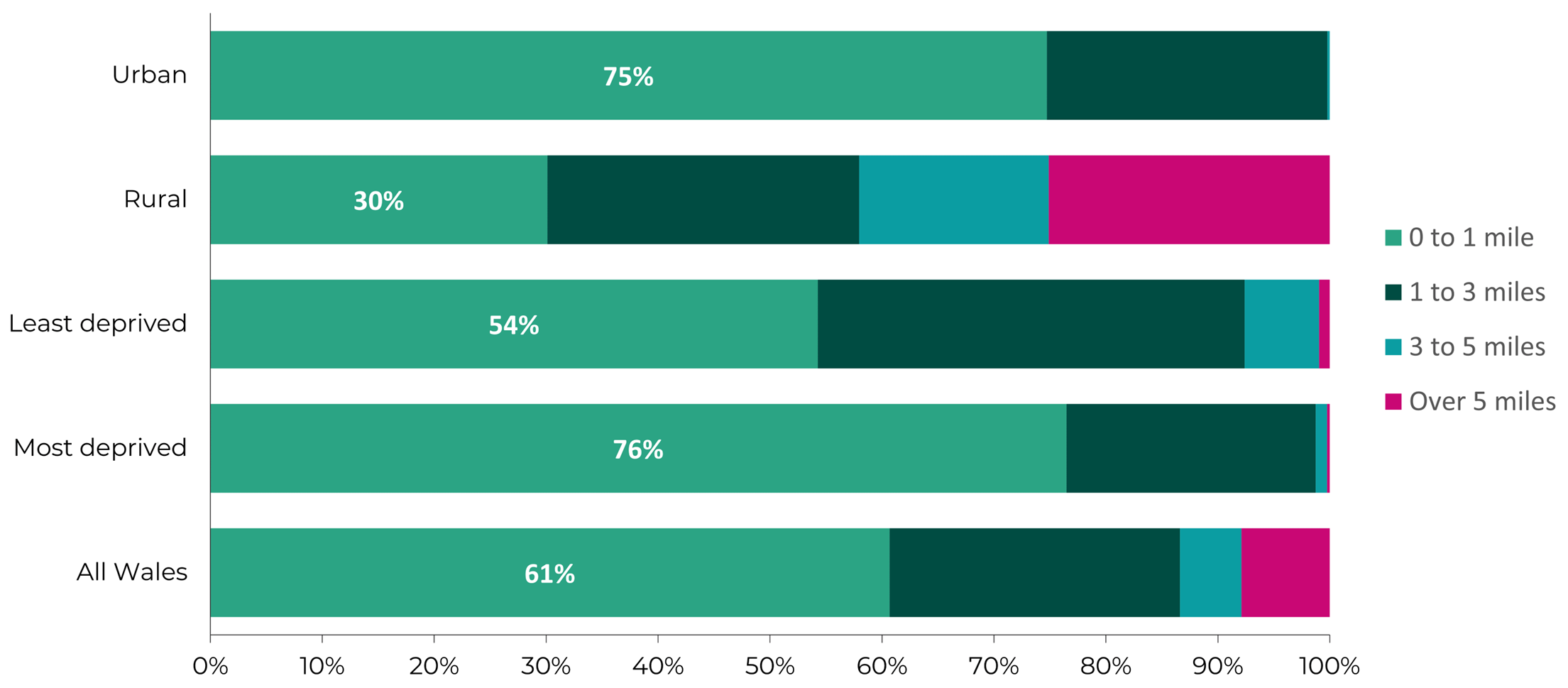
Sources: General Dental Practices data, Mid-year population estimates 2020, Welsh Index of Multiple Deprivation 2019, ONS Rural-urban classification.
Figure 4 (above) shows that most people in Wales (61%) live within 1 mile of their nearest dental practice. Unsurprisingly, rural residents tend to live further from the nearest dental practice, with 25% of rural residents travelling more than 5 miles to the nearest practice. Residents of the most deprived areas, which tend to be in urban areas, have better physical access to dental practices than people in the least deprived areas.
Figure 5: Travel distance to the nearest NHS dental practice
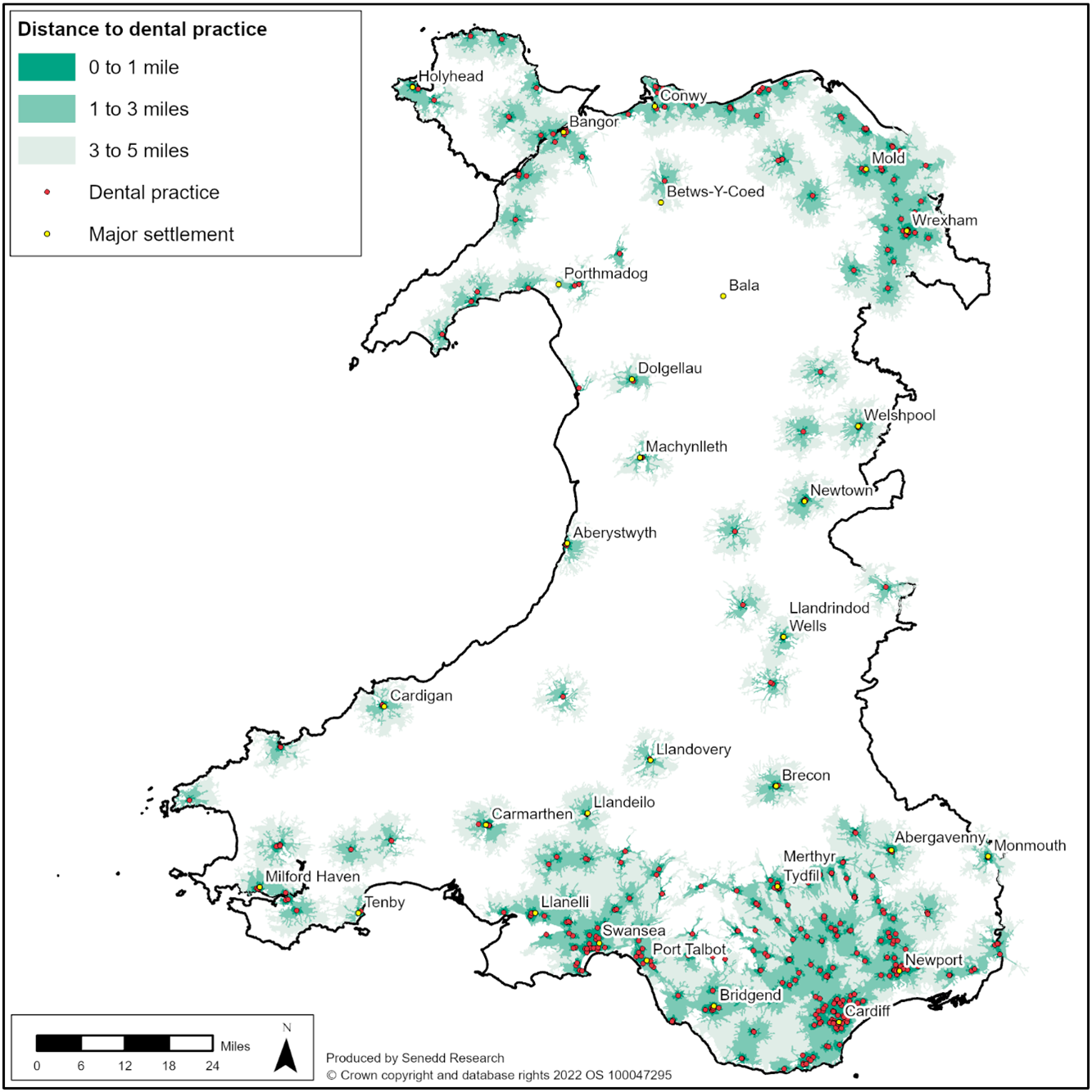
Sources: General Dental Practices , Mid-year population estimates 2020, Welsh Index of Multiple Deprivation 2019, ONS Rural-urban classification, Road network. Distances reflect actual travel distance along the road network.
Beyond simple measures of distance, analysis by population groups in terms of who can access and afford dental treatment isn’t possible. The data also doesn’t include vulnerable groups that may access dental care through Community Dental Services (explored further in our second article). To better understand access to dental care through an equality lens, integrated General Dental Service (GDS) and Community Dental Services (CDS) databases and analyses is needed.
Article by Katie Devenish, Sarah Hatherley and Sam Jones Senedd Research, Welsh Parliament
