


Medicines shortages and rising prices have become a persistent challenge for health services across the UK, including in Wales.
While the causes are largely global, and responsibility for maintaining the continuity of medicines supply rests with the UK Government, the consequences are felt by patients, prescribers, and community pharmacies across Wales.
This article examines which medicines are affected by shortages, the factors contributing to shortages and rising prices, and the position in Wales.
Which medicines have been affected by shortages?
The number of medicines affected by shortages in the UK reached a peak in 2024 before falling in 2025. Since the beginning of 2026, however, the number has begun to rise again.
Average number of weekly medicines shortages in the UK
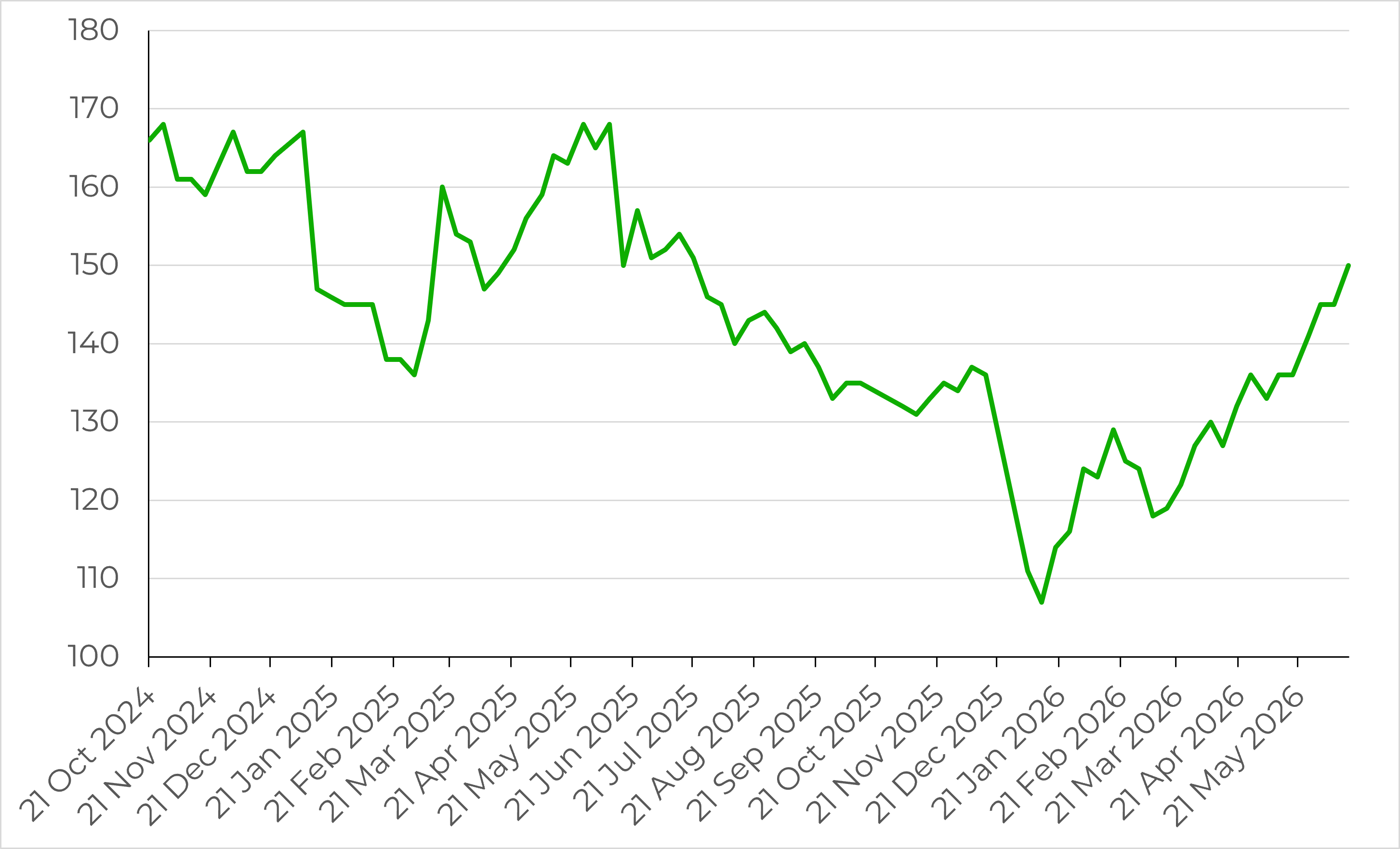
Source: MIMS Healthcare Network
Supply disruptions usually affect only a small fraction of medicines at any time, but the impact on patients where there is no clinical alternative can be significant.
One example is pancreatic enzyme replacement therapy (PERT), primarily the brand Creon®, used by people with pancreatic cancer, cystic fibrosis, and chronic pancreatitis to support digestion. The shortage has been significant enough to trigger a Serious Shortage Protocol (SSP)—a formal UK Government measure that provides guidance to community pharmacists on supplying clinically appropriate alternatives.
SSPs for Creon® have been in place since May 2024, and the shortage is expected to continue until 2027. While alternative PERT products do exist, they are not always interchangeable or readily available, and some patients have reported eating only one meal a day to ration capsules.
Parkinson’s UK has also warned of supply issues affecting a number of Parkinson's medicines into mid and late 2026. For people with Parkinson's, the impact can be considerable, as switching between brands can trigger a return of symptoms.
Other recent examples include medicines used to treat ADHD, epilepsy, and type 2 diabetes. Supply constraints have also impacted widely prescribed medicines such as aspirin, co‑codamol and ramipril, indicating that shortages are not confined to specialist medicines.
What is driving medicines shortages?
Medicine supply chains are global, highly regulated and complex, and shortages are a worldwide problem. The following are some of the most commonly cited drivers.
Concentrated overseas manufacturing
The UK depends heavily on overseas production of medicines and the active pharmaceutical ingredients (APIs) used to make them. A February 2026 report by the House of Lords Public Services Committee found that most APIs used in NHS medicines are sourced from China, India, or other single sources. It also noted that although generic medicines account for around 80% of NHS prescriptions, only about a quarter are manufactured in the UK, with the majority produced elsewhere in Europe and Asia.
A single factory closure, regulatory breach, or transport delay in these manufacturing hubs can therefore quickly affect UK availability. Most disruptions notified to the Department of Health and Social Care (DHSC) are attributed to issues at the manufacturing stage.
Geopolitical shocks
The COVID-19 pandemic, the war in Ukraine, and disruption in the Strait of Hormuz linked to the Iran conflict have all exposed UK reliance on long international supply chains. The Iran conflict is reported to have raised the cost of some prescription medicines by around 30%, largely through higher petrol and diesel prices that flow through to manufacturing and shipping costs.
Surges in demand
Demand can outpace manufacturers' capacity to scale up. Prescribing of hormone replacement therapy (HRT) rose by more than 90% in Wales between 2015 and 2022, partly driven by awareness campaigns, resulting in repeated shortages of menopause treatments.
The rapid uptake of GLP-1 agonists such as semaglutide for weight loss has similarly constrained global supply.
New diagnoses, changes to clinical guidelines, and media coverage can all trigger sudden shifts in demand that producers cannot match quickly.
Commercial pressures
Spending on medicines makes up a smaller proportion of total health expenditure in the UK than in comparable countries, and industry bodies have argued this reduces the incentive for suppliers to prioritise the UK market over more profitable destinations. In 2025, AstraZeneca, Eli Lilly, and MSD (Merck) paused or withdrew planned UK investments which were worth almost £2 billion between them.
The UK Government has acknowledged that low pricing can create risks for the long-term resilience of medicines supply. More recently, the UK-US Economic Prosperity Deal has been linked to some renewed investment in the sector.
Regulatory barriers
Since 2021, the Medicines and Healthcare products Regulatory Agency (MHRA) has authorised new medicines separately from the European Medicines Agency. Approval times have typically been slower, which may reduce the range of alternative products available when shortages occur.
Why are medicine prices rising?
Many of the same pressures driving shortages also push up the price of medicines, particularly in the generic medicines market. Unlike branded medicines, generic prices are not subject to a UK-wide cap and can fluctuate significantly with global market conditions.
In April 2026, the National Pharmacy Association warned that the cost of some commonly prescribed medicines had risen 14 to 15 times since the start of the year, with a pack of 100 paracetamol tablets rising from 41p to £1.99 by the end of March.
These price rises have placed significant pressure on community pharmacies. The prices pharmacies are reimbursed for dispensing NHS prescriptions are set out in the monthly Drug Tariff, which sets a fixed reimbursement rate for each medicine and applies in both England and Wales. When the open-market price a pharmacy pays for a medicine rises above the Drug Tariff rate, the pharmacy is left dispensing at a loss. The National Pharmacy Association has reported that the NHS can pay as little as 20% of the cost of some commonly dispensed medicines.
Community Pharmacy Wales can request a price concession from the Welsh Government to bridge the gap, which adjusts reimbursement upward for the month it is granted. Even with this mechanism in place, the Company Chemists' Association has reported that four in ten Welsh pharmacies were unprofitable in 2025. According to the National Pharmacy Association, 60% of pharmacy owners in Wales had remortgaged their house or used personal savings to stay open in the last year.
What is the position in Wales?
Responsibility for maintaining the continuity of medicines supply to the UK is reserved to the UK Government, while responsibility for managing the impact of any disruptions on patients in Wales is devolved. The levers available to the Welsh Government to address the underlying causes of shortages are therefore limited.
When supply issues arise, Welsh Government officials work with UK counterparts, regulators, the pharmaceutical industry and NHS Wales to minimise disruptions. In a September 2024 written statement, the then Cabinet Secretary for Health and Social Care attributed improvements in the supply of ADHD and HRT medicines partly to this coordination work.
The Chief Pharmaceutical Officer for Wales also issues medicines shortage letters to GPs and pharmacies when new issues emerge, providing clinical advice on alternative treatments.
For patients, the Welsh Government maintains a dedicated medicines shortages webpage with information on specific medicines, reasons for shortages, and expected resolution dates. The All Wales Therapeutics and Toxicology Centre (AWTTC) has also published patient information leaflets on managing shortages.
Medicines shortages and price pressures are unlikely to ease significantly in the near term. The Welsh Government can coordinate the response within Wales, provide advice to clinicians, and make information available to patients, but the underlying causes of disruption, and the powers needed to address them, sit largely outside its control. The consequences, however, will continue to be felt in Wales.
Article by John Hitchcock, Senedd Research, Welsh Parliament
