


This article is published as part of the Assembly’s pilot Academic Fellowship Scheme, which enables academics to work at the Assembly on a specific project, for the mutual benefit of the academic and the Assembly. Professor John’s work here will particularly help inform the Health, Social Care and Sport Committee’s current inquiry into suicide prevention.
Every suicide is a tragedy and causes distress for family, friends, professionals and the wider community. Although the factors that contribute to a suicide are many and complex, suicide is potentially preventable. Knowing who dies by suicide and when is essential to suicide prevention efforts, since it allows us to identify changes over time, enabling responsive priorities to be set to inform policy and practice and document the impact of any interventions. In Wales there are a number of sources of information on suicide but two important ones are data from the Office of National Statistics provided by Public Health Wales and the Suicide Information Database-Wales (SID-Cymru), based at Swansea University and part funded by Health and Care Research Wales through the National Centre for Mental Health.
Suicide data for Wales
A detailed analysis of data in Wales is being produced for the mid-point review of Talk to Me , the current Wales strategy for suicide and self-harm prevention. In Wales there were 322 suicides in those aged 10 years and over in 2016, 28 less than the 350 recorded in 2015 but 75 higher than the 247 recorded in 2014. In 2013 there were 393 suicides in Wales, the highest recorded figure since 2002.
Wales in comparison with other UK nations
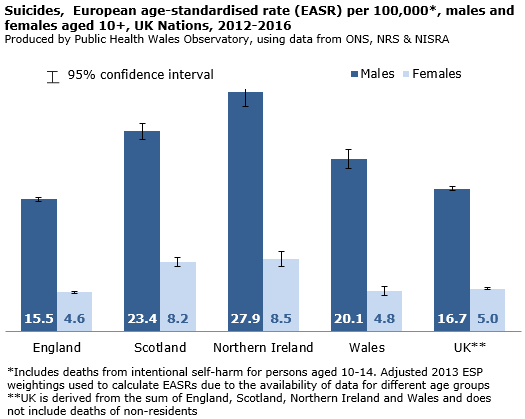
There are differences in coding in Scotland and Northern Ireland, so comparisons across the United Kingdom nations should be interpreted with caution.
The rate of suicide in Wales (2012-2016) was higher than that of the UK average for males (Figure 1) but equivalent for females. Figure 1
SID-Cymru
SID-Cymru anonymously links, at an individual level, electronic routinely collected data about all persons in Wales, over 10 years of age, who were recorded to have died by suicide between 1 January 2001 and 31 December 2015. Currently the focus is on the prior health, nature of previous contacts with services and wider social circumstances of all those who die through suicide (known and unknown to mental health services) to inform prevention, policy and practice.
This study, for the first time in the United Kingdom, links routinely collected primary care, emergency department attendance and hospital admissions at a whole population level to identify patterns of service contact for those who die by suicide prior to their deaths. There is a particular focus in this project on the opportunities for prevention in primary care and emergency departments. Data from SID-Cymru informed the Thematic review of deaths of children and young people through probable suicide, 2006-2012. The review made a number of recommendations to various agencies, such as minimum unit pricing for alcohol and on the care of under 18 year olds with alcohol related or self – harm emergency department attendances. A repeat review is being conducted this year. 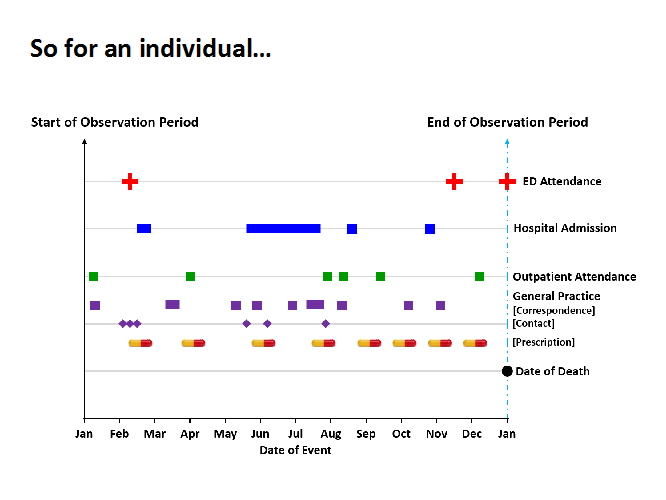
A total of 4289 people resident in Wales who died by suicide, with a date of death from 2001-2015, are currently included in SID-Cymru each with 10 controls of the same age and sex who were alive on their date of death. Just over three-quarters of those who died by suicide were male, which is in keeping with the research literature. There was a socio-economic gradient in those who died by suicide (14% from the least deprived quintile of area deprivation and 26% from the most deprived) which was not evident in controls. This highlights that activities preventing suicide need to address inequalities. Those who died by suicide had contact with their GP as much as those who did not in the year prior to their deaths but this was more likely to be for mental health problems (19% vs. 4%) or self-harm (7% vs. 0.2%).
SID-Cymru provides evidence that suicide prevention activities need to occur across all health settings not just in mental health services. Increased awareness is required for all priority care providers. However, it also highlights that over a quarter of those who die by suicide have had contact with mental health services in the year prior to their death. For this reason SID-Cymru has partnered with the National Confidential Inquiry into Suicide and Homicide to link to SID-Cymru the in-depth questionnaire data they hold on those people in Wales who had contact with mental health services in the year prior to their deaths with the aim of identifying further risk factors.
No single organisation or sector can prevent suicide in isolation. In the future it is planned to link the health data in SID-Cymru with further social care and other priority care provider data creating a huge resource to inform prevention efforts, policy and practice in Wales so fewer people die by suicide. 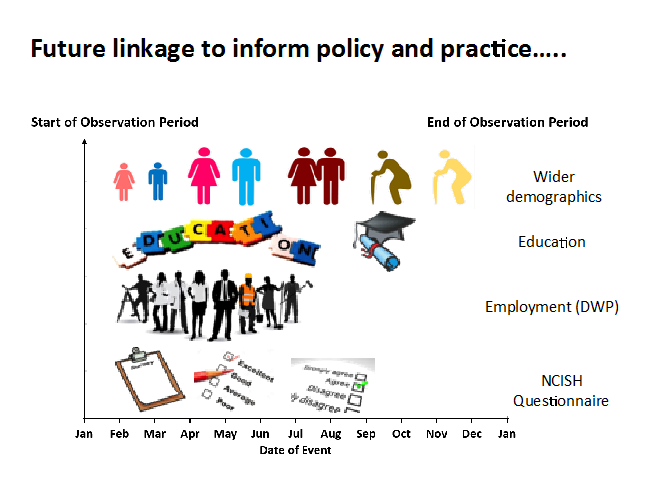
Understanding suicide data
There are a number of issues to consider when thinking about what suicide statistics mean:
Definitions
Everything presented here refers to the Office for National Statistics (ONS) classification of suicide. In this definition suicide includes where the underlying cause of death was intentional self-harm or an event of undetermined intent.
In 2016, the National Statistics definition of suicide was modified to include deaths from intentional self-harm in 10 to 14 year old children in addition to deaths from intentional self-harm and events of undetermined intent in people aged 15 and over.
Under-reporting of suicide
It is widely acknowledged that official statistics may underestimate the ‘true’ numbers of suicide in the United Kingdom and across the world. Deaths may be misclassified where a coroner cannot establish that the intent of the individual was to take their own life. Where such a death is recorded as ‘undetermined intent’ it will be included in suicide statistics but where it is coded as accidental it will not. The latter occurs, for example, in single vehicle road traffic accidents.
Coroners record a conclusion of suicide based on the principle of ‘beyond doubt’ rather than ‘balance of probabilities’. This may be difficult to determine. Stigma may also play a role when assigning a cause of death as suicide.
Narrative verdicts
It should be noted that following a coroner's inquest into a death, the coroner may decide to use a narrative verdict to report their conclusions as to the cause of death. Some narrative verdicts do not specify whether the fatal injury was accidental or involved deliberate intent to self-harm. The ONS call these verdicts 'hard-to-code'. Following concern about an upward trend in 'hard-to-code' narrative verdicts, with numbers increasing in Wales from 52 in 2006 to 147 in 2010, ONS took action by providing both their own coding staff and also coroners with additional guidance on narrative verdicts. These actions appear to be having a positive impact, with ONS reporting a 49% drop in hard-to-code narrative verdicts in Wales between 2010 and 2011 registrations. However a reduction in the number of hard-to-code narrative verdicts could lead to an apparent rise in the numbers of suicides from 2011 onwards, when in fact the rise could be partly due to improved reporting from coroners and improved coding by ONS. Conversely reported numbers of suicides are likely to be underestimated, particularly between 2006 and 2010.
Delays in registration
Official data are subject to delay in availability. Before a suicide death can be registered an inquest must be completed (England and Wales); the length of time for this from death is variable. For this reason the information provided by Public Health Wales is presented by year of registration rather than year of death whereas that from SID-Cymru is by year of death.
Year on year fluctuations
When looking at trends over time it’s important to look over a relatively long period not any one year in isolation. There will be year on year fluctuations that are unlikely to be a reflection of ‘true’ changes in trends.
Small populations
Where populations are small, for example where males and females are analysed separately, rates can be unreliable since a small change in the number of suicides will have a large impact on rates. When this occurs it is demonstrated by relatively wide confidence intervals (bars around points in graphs, ranges in brackets). In these analyses any comparisons should be interpreted with caution and particular attention paid to overlapping error bars where differences are then not statistically significant i.e. we cannot really say there is a ‘true’ difference.
Age standardised vs. crude rates
Age standardised rates have been standardised to the European population so comparisons can be made. This is because the age structure of a population impacts rates i.e. if looking at stroke one area may contain a higher proportion of older people so rates would be higher but this would be expected. Crude rates are not standardised in this way.
Article by Ann John, Professor of Public Health and Psychiatry, Swansea University Medical School
